
A new study looks at the connection between air pollution and health by focusing on emergency room visits for cardiovascular and respiratory diseases in five cities, Atlanta, Birmingham, Dallas, St. Louis, and Pittsburgh.
One of the takeaways the researchers found was that primary pollutants — ones that come directly from a source (car exhaust for example) — were linked with emergency room visits for cardiovascular and respiratory diseases. And secondary pollutants — ones that are caused by chemical reactions in the air (ozone for example) — were associated to emergency room visits for respiratory diseases.
Evelyn Talbott, professor of epidemiology at the Graduate School of Public Health at the University of Pittsburgh contributed to the study. She says it incorporates data from 48 air monitors in the greater Pittsburgh region, and data from the area’s major health care providers.
Kara Holsopple spoke with Talbott recently to learn more.
Kara Holsopple: This study looked at a number of types of air pollution in several cities and their links to emergency room or doctor’s visits. What are some of the main takeaways?
Evelyn Talbott: The uniqueness of this [study] is that you have five cities and 12 pollutants so you are able to look at a whole lot of ER visits. They were able to not just look at one pollutant and one effect; they are able to combine them and look at groups. They didn’t just look at asthma or heart attack…they looked at all cardiac diseases: congestive heart failure, arrhythmia, ischemic heart disease, stroke. And they also looked at respiratory diseases: COPD, bronchitis, exacerbations, asthma.
They also asked where are the worst culprits [in terms of air pollution and ER visits]. They actually found that congestive heart failure had a very significant effect with nitrogen dioxide (NO2), something that is related to the burning of gasoline, coal or natural gas.
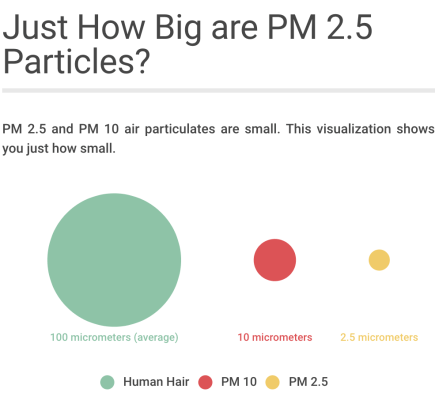
On high PM 2.5 days [particulate matter 2.5 microns or smaller], there’s a tendency for people who are already vulnerable — already have asthma, already have congestive heart failure, already have COPD — they’re more susceptible.
LISTEN to the interview:
Holsopple: Specific to Pittsburgh, were there any findings that are interesting?
Talbott: We have a lot of cars, but we also have we have a lot of industry. Pittsburgh does not have as high of an ozone level as let’s say Atlanta, Birmingham or Dallas. They had higher ozone which doesn’t really surprise me so much for Atlanta and Dallas. Why? Because it’s warmer. Pittsburgh was 37 parts per billion (ppb) compared to 41.
But for other pollutants, Pittsburgh was higher. For example, NO2 was 26 ppb compared to the others that were between 13 and 21 ppb. And that’s because NO2 is related to the burning of coal and industry.
PM 10 was pretty close to Birmingham. And PM 2.5 was even-steven with Atlanta. Elemental carbon, organic carbon, sulphate — they were all the highest. This was 2002 to 2008. I would hope that we’re doing better than we were, but at that point we did have very high air pollution levels.
Holsopple: And what does that mean for the health of people who live in this region?
Talbott: There were relationships between stroke, congestive heart failure, asthma and these various pollutants. So I would say that it is a very good thing that from 2002 to 2008/9, our air pollution has probably gone down another 15 or 20 percent.
Holsopple: Does this study tell us anything about the Pittsburgh region’s air quality and how it affects people that we didn’t already know?
Talbott: I think what it shows is that 10 years ago (2002-2008), we certainly had higher levels than some of these major cities like Atlanta and Dallas. Yes, they have a lot of cars, but perhaps there were doing a better job with some of the other industry that they have.
Going forward, what it says to me is we do continue to see an effect on congestive heart failure, on asthma, on children. And so we have to continue to make some strides because we clearly have to do better than we’re doing now.
Holsopple: How could a study like this be used for setting air pollution standards by the U.S. EPA. Or can it? How does it help move the needle?
Talbott: The fact that there are 12 pollutants [in this study] I think really does push the needle because when you’re setting a standard, can you really set that standard in a vacuum? Can you really say just that pollutant, and no other pollutant, has to be regulated? Absolutely not. This really shows me that you should really be looking at it in tandem.
I can’t imagine EPA funding another study without the applicability of looking at multiple pollutants when possible. You know, PM 2.5 isn’t just a lump of soot; there are a lot of other little molecules and chemicals in there. So more and more people are interested in the big picture, but these elemental speciation of these various sub chemicals is probably going to end up being more important. Different places have different kinds of PM 2.5. If you go to Florida, you have a lot of silica. Why? Because there’s a lot of sand.
So I think it is important to see where the health effects are related to these subspecies. I think that’s where the field is going.
###
Related video about soot pollution – how other chemicals in the air attach to soot particles.
